Introduction
The chief concern over laser use has always been the possibility of eye injury. While skin presents a greater target, it is injury to one’s eyes that drives laser safety, funding, controls and application. The effect of laser radiation will vary with the wavelength and part of the eye it interacts with. In addition biological effects from direct exposure and diffuse reflection exposure will differ. The anatomy of the eye and skin will be explained and issues associated with biological effects.
Exposure Type
One of the deciding factors on how hazardous a laser beam can be is how one is exposed. Is it a direct or intrabeam exposure (where all the energy is directed right at one’s eyes).
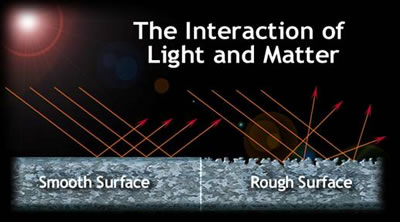
A specular reflection, which is a reflection off a mirror like surface (keeping in mind different surfaces to different wavelengths may or may not be mirror like. Specular reflection will result when the surface roughness is smaller than the wavelength. Specular reflections are generally less than 100%.
The safest reflection is the diffuse reflection, a reflection off a surface that spreads out the laser radiation reducing its irradiance. A diffuse surface will be one where the surface roughness is larger that the wavelength.
The Eye
The major danger of laser radiation is hazards from beams entering the eye. The eye is the organ most sensitive to light. A laser beam (400-1400 nm) with low divergence entering the eye can be focused down to an area 10 to 20 microns in diameter.
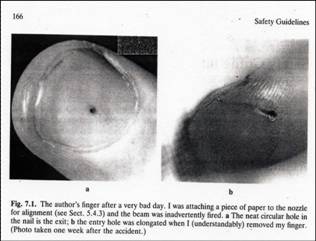
The energy density (measure of energy per unit of area) of the laser beam increases as the spot size decreases. This means that the energy of a laser beam can be intensified up to 100,000 times by the focusing action of the eye for visible and near infrared wavelengths. If the irradiance entering the eye is 1 mW/cm2, the irradiance at the retina will be 100 W/cm2. Even a 4% reflection off an optic can be a serious eye hazard. Remember a low power laser in the milliwatt range can cause a burn if focused directly onto the retina. A 40 mW laser is capable of producing enough energy (when focused) to instantly burn through paper.
The path of visible light
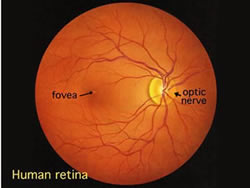
Light from an object (such as a tree) enters the eye first through the clear cornea and then through the pupil the circular aperture (opening) in the iris. Next, the light is converged by the lens to a nodal point immediately behind the lens; at that point, the image becomes inverted. The light progresses through the gelatinous vitreous humor and, ideally, back to a clear focus on the retina, the central area of which is the macula. In the retina, light impulses are changed into electrical signals and then sent along the optic nerve and back to the occipital (posterior) lobe of the brain, which interprets these electrical signals as visual images
Major parts of the human eye
The cornea is the transparent layer of tissue covering the eye. Damage to the outer cornea may be uncomfortable (like a gritty feeling) or painful, but will usually heal quickly. Damage to deeper layers of the cornea may cause permanent injury.
The lens focuses light to form images onto the retina. Over time, the lens becomes less pliable, making it more difficult to focus on near objects. With age, the lens also becomes cloudy and eventually opacifies. This is known as a cataract. Every lens develops cataracts eventually.
Retina
The part of the eye that provides the most acute vision is the fovea centralis (also called the macula lutea). This is a relatively small area of the retina (3 to 4%) that provides the most detailed and acute vision as well as color perception. This explains why eyes move when you read the image has to be focused on the fovea for detailed perception. The balance of the retina can perceive light and movement.
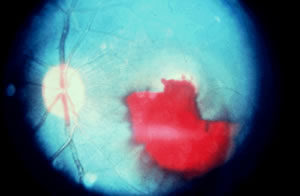
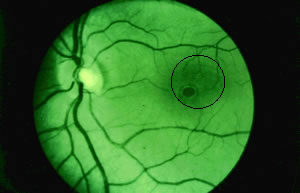
If a laser burn occurs on the fovea, most fine (reading and working) vision may be lost. If a laser burn occurs in the peripheral vision, it may produce little or no effect on vision.
Blink and aversion response
Fortunately the eye has a self-defense mechanism — the blink and aversion response. Aversion response is the closing of the eyelid, or movement of the head to avoid exposure to bright light. The aversion response is commonly assumed to occur within 0.25 sec and is only applicable to visible laser wavelengths. This response may defend the eye from damage where lower power lasers are involved, but cannot help where higher power lasers are involved. With high power lasers, the damage can occur in less time than a quarter of a second.
The study “A Critical Consideration of the Blink Reflex as a Means for Laser Safety Regulations, byH.-D. Reidenbach1,2,3, J. Hofmann1, K. Dollinger1,3, M. Seckler2.
This study states that even for the larger spot size on the retina the frequency of the blink reflex has been shown to be less than 35 % and the same is true for the maximum of the pupil size, i. e. for low ambient light conditions. The study states 503 volunteers have been irradiated in the lab and 690 in 4 different field trials with laser radiation. Out of these only 15.5 % or 18.26 % respectively have shown a blink reflex. The respective numbers as a function of wavelength are: 15.7 % (670 nm), 17.2 % (635 nm), and 22.4 % (532 nm). An increase from 4.2 % up to 28.1 % in blink reflex frequency was achieved when the ambient illuminance was decreased from 1 700 lx to 1 lx using an LED as a large extended stimulating optical source instead of a collimated laser beam.
A further dependency was found concerning the irradiated area on the retina, i.e. increasing the retinal spot from 6.4 to 9.4 mm2 up to 33.7 to 46.8 mm2 resulted in an increase of the blink reflex percentage from 20 % to 33.3 %.
Effects are wavelength-dependent
Ultraviolet-B+C (100 – 315 nm)
The surface of the cornea absorbs all UV of these wavelengths which produce a photokeratitis (welders flash) by a photochemical process, which cause a denaturation of proteins in the cornea. This is a temporary condition because the corneal tissues regenerate very quickly.
Ultraviolet -A (315 – 400 nm)
The cornea, lens and aqueous humour allow Ultraviolet radiation of these wavelengths and the principal absorber is the lens. Photochemical processes denature proteins in the lens resulting in the formation of cataracts.
Visible light and Infrared-A (400 – 1400 nm)
The cornea, lens and vitreous fluid are transparent to wavelengths. Damage to the retinal tissue occurs by absorption of light and its conversion to heat by the melanin granules in the pigmented epithelium or by photochemical action to the photoreceptor. The focusing effects of the cornea and lens will increase the irradiance on the retina by up to 100,000 times. For visible light 400 to 700 nm the aversion reflex which takes 0.25 seconds may reduce exposure causing the subject to turn away from a bright light source. However, this will not occur if the intensity of the laser is great enough to produce damage in less than 0.25 sec. or when light of 700 – 1400 nm (near infrared) is used, as the human eye is insensitive to these wavelengths.
Infrared-B and Infrared-C (1400 to 1.0 x 10+6 nm)
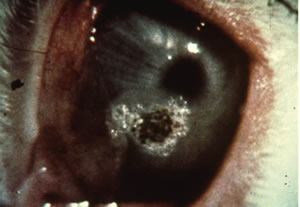
Corneal tissue will absorb light with a wavelength longer than 1400 nm. Damage to the cornea results from the absorption of energy by tears and tissue water causing a temperature rise and subsequent denaturation of protein in the corneal surface.
Signs of Eye Exposure
Symptoms of a laser burn in the eye include a headache shortly after exposure, excessive watering of the eyes, and sudden appearance of floaters in your vision. Floaters are those swirling distortions that occur randomly in normal vision most often after a blink or when eyes have been closed for a couple of seconds. Floaters are caused by dead cell tissues that detach from the retina and choroid and float in the vitreous humor. Ophthalmologists often dismiss minor laser injuries as floaters due to the very difficult task of detecting minor retinal injuries. Minor corneal burns cause a gritty feeling, like sand in the eye.
The exposure to a visible laser beam can be detected by a bright color flash of the emitted wavelength and an after-image of its complementary color (e.g., a green 532 nm laser light would produce a green flash followed by a red after-image). When the retina is affected, there may be difficulty in detecting blue or green colors secondary to cone damage and pigmentation of the retina may be detected.
Exposure to the Q-switched Nd:YAG laser beam (1064 nm) is especially hazardous and may initially go undetected because the beam is invisible and the retina lacks pain sensory nerves. Photoacoustic retinal damage may be associated with an audible “pop” at the time of exposure. Visual disorientation due to retinal damage may not be apparent to the operator until considerable thermal damage has occurred.

Exposure to the invisible carbon dioxide laser beam (10,600 nm) can be detected by a burning pain at the site of exposure on the cornea or sclera.
Damage Mechanisms
Electromechanical/Acoustic Damage
This type of damage requires beams of extremely high power density (109–1012 W/cm2) in extremely short pulses (ns) to delivery fluences of about 100 J/cm2 and very high electric fields (106–107 V/cm), comparable to the average atomic or intermolecular electric field. Such a pulse induces dielectric breakdown in tissue, resulting in a microplasma or ionized volume with a very large number of electrons. A localized mechanical rupture of tissue occurs due to the shock wave associated with the plasma expansion. Laser pulses of less than 10 microseconds duration can induce a shock wave in the retinal tissue that causes tissue rupture. This damage is permanent, as with a retinal burn. Acoustic damage is actually more destructive to the retina than a thermal burn. Acoustic damage usually affects a greater area of the retina, and the threshold energy for this effect is substantially lower. The ANSI MPE values are reduced for short laser pulses to protect against this effect.
Photoablation
Photoablation is the photodissociation or direct breaking of intramolecular bonds in biopolymers, caused by absorption of incident photons and subsequent release of biological material. Molecules of collagen, for example, may dissociate by absorption of single photons in the 5–7 eV energy range. Excimer lasers at several ultraviolet wavelengths (ArF, 193 nm/6.4 eV; KrF, 248 nm/5 eV; XeCl, 308 nm/4 eV) with nanosecond pulses focused on tissue at power densities of about 108 W/cm2 can produce this photoablative effect. Ultraviolet radiation is extremely strongly absorbed by biomolecules, and thus absorption depths are small, of the order of a few micrometers.
Thermal Damage

Thermal damage occurs because of the conversion of laser energy into heat. With the laser’s ability to focus on points a few micrometers or millimeters in diameter, high power densities can be spatially confined to heat target tissues. Depth of penetration into the tissue varies with wavelength of the incident radiation, determining the amount of tissue removal and bleeding control.
The photothermal process occurs first with the absorption of photon energy, producing a vibrational excited state in molecules, and then in elastic scattering with neighboring molecules, increasing their kinetic energy and creating a temperature rise. Under normal conditions the kinetic energy per molecule (kT) is about 0.025 eV. Heating effects are largely controlled by molecular target absorption such as free water, haemoproteins, melanin, and other macromolecules such as nucleic acids.
Photochemical Damage
Light below 400 nm does not focus on the retina. The light can be laser output, ultraviolet (UV) from the pump light, or blue light from a target interaction. The effect is cumulative over a period of days. The ANSI standard is designed to account only for exposure to laser light. If UV light from a pump light or blue light from a target interaction is emitted, additional precautions must be taken.
Key Advice: DO NOT look directly into the beam.
Laser Radiation Effects on Skin
Laser radiation injury to the skin is normally considered less serious than injury to the eye, since functional loss of the eye is more debilitating than damage to the skin, although the injury thresholds for both skin and eyes are comparable (except in the retinal hazard region, (400–1,400 nm). In the far-infrared and far-ultraviolet regions of the spectrum, where optical radiation is not focused on the retina, skin injury thresholds are about the same as corneal injury thresholds. Obviously, the possibility of skin exposure is greater than that of eye exposure because of the skin’s greater surface area.
The layers of the skin, which are of concern in a discussion of laser hazards to the skin, are the epidermis and the dermis. The epidermis layer lies beneath the stratum corneum and is the outermost living layer of the skin. The dermis mostly consists of connective tissue and lies beneath the epidermis.
Epidermis
The epidermis is the outer layer of skin. The thickness of the epidermis varies in different types of skin. It is the thinnest on the eyelids at .05 mm and the thickest on the palms and soles at 1.5 mm.
Dermis
The dermis also varies in thickness depending on the location of the skin. It is .3 mm on the eyelid and 3.0 mm on the back. The dermis is composed of three types of tissue that are present throughout – not in layers. The types of tissue are collagen, elastic tissue, and reticular fibers.
Subcutaneous Tissue
The subcutaneous tissue is a layer of fat and connective tissue that houses larger blood vessels and nerves. This layer is important is the regulation of temperature of the skin itself and the body. The size of this layer varies throughout the body and from person to person.
There is quite a variation in depth of penetration over the range of wavelengths, with the maximum occurring around 700 to 1200 nm. Injury thresholds resulting from exposure of less than 10 seconds to the skin from far-infrared and far-ultraviolet radiation are superficial and may involve changes to the outer dead layer of the skin. A temporary skin injury may be painful if sufficiently severe, but it will eventually heal, often without any sign of injury. Burns to larger areas of the skin are more serious, as they may lead to serious loss of body fluids. Hazardous exposure of large areas of the skin is unlikely to be encountered in normal laser work.
A sensation of warmth resulting from the absorption of laser energy normally provides adequate warning to prevent thermal injury to the skin from almost all lasers except for some high-power far-infrared lasers. Any irradiance of 0.1 W/cm2 produces a sensation of warmth at diameters larger than 1 cm. On the other hand, one tenth of this level can be readily sensed if a large portion of the body is exposed. Long-term exposure to UV lasers has been shown to cause long-term delayed effects such as accelerated skin aging and skin cancer.
To the skin, UV-A (0.315 µm-0.400 µm) can cause hyperpigmentation and erythema. UV-B and UV-C, often collectively referred to as “actinic UV,” can cause erythema and blistering, as they are absorbed in the epidermis. UV-B is a component of sunlight that is thought to have carcinogenic effects on the skin. Exposure in the UV-B range is most injurious to skin. In addition to thermal injury caused by ultraviolet energy, there is the possibility of radiation carcinogenesis from UV-B (280 nm – 315 nm) either directly on DNA or from effects on potential carcinogenic intracellular viruses.
Exposure in the shorter UV-C (0.200 µm-0.280 µm) and the longer UV-A ranges seems less harmful to human skin. The shorter wavelengths are absorbed in the outer dead layers of the epidermis (stratum corium) and the longer wavelengths have an initial pigment-darkening effect followed by erythema if there is exposure to excessive levels.
IR-A wavelengths of light are absorbed by the dermis and can cause deep heating of skin tissue.